Get Prescription Pad Form in PDF
The Prescription Pad form serves as a crucial tool in the healthcare landscape, streamlining the process of prescribing medication while ensuring patient safety and compliance with regulatory standards. This form typically includes essential information such as the patient's name, date of birth, and medication details, including dosage and administration instructions. By standardizing the prescription process, healthcare providers can minimize errors and enhance communication with pharmacies. Additionally, the form often incorporates sections for the prescriber’s information, allowing for easy verification of credentials and contact details. Its design may also include fields for refills, ensuring that patients have a clear understanding of their medication regimen. Ultimately, the Prescription Pad form is more than just a piece of paper; it represents a vital link between patients and their healthcare providers, fostering a relationship built on trust and clarity in medication management.
Dos and Don'ts
When filling out a Prescription Pad form, it is essential to ensure accuracy and compliance with regulations. Here are some important guidelines to follow:
- Do ensure that all patient information is complete and accurate.
- Do write legibly to avoid any misunderstandings regarding the medication prescribed.
- Do include the date on which the prescription is written.
- Do specify the dosage and frequency clearly.
- Don't use abbreviations that could be misinterpreted.
- Don't leave any sections of the form blank, as this could lead to confusion or delays in treatment.
Document Attributes
| Fact Name | Description |
|---|---|
| Purpose | The Prescription Pad form is used by healthcare providers to prescribe medications to patients, ensuring proper documentation and compliance with medical regulations. |
| State-Specific Regulations | Each state has its own regulations governing the use of prescription pads, often requiring specific information to be included, such as the prescriber's license number and the patient's details. |
| Security Features | Prescription pads typically include security features to prevent forgery and unauthorized use, such as watermarks or unique serial numbers. |
| Record Keeping | Healthcare providers are required to maintain records of all prescriptions issued, which may be subject to audits by regulatory bodies to ensure compliance with state and federal laws. |
Key takeaways
When filling out and using the Prescription Pad form, there are several important aspects to consider. Here are nine key takeaways:
- Accurate Information: Ensure that all patient details, including name, address, and date of birth, are entered correctly to avoid any confusion.
- Medication Details: Clearly specify the medication name, dosage, and frequency. This helps pharmacists dispense the correct medication.
- Signature Requirement: The prescribing physician must sign the prescription. An unsigned prescription may not be valid.
- Refill Instructions: Indicate whether refills are allowed and how many. This information is crucial for ongoing patient care.
- Controlled Substances: If prescribing controlled substances, ensure compliance with state and federal regulations. Special forms may be required.
- Patient Instructions: Provide clear instructions for the patient regarding medication use and potential side effects.
- Emergency Contact: Include an emergency contact number for any questions or concerns that may arise after the prescription is filled.
- Record Keeping: Maintain a copy of the prescription for your records. This can be important for follow-up and accountability.
- Timely Updates: If there are any changes to the patient's condition or medication needs, update the prescription promptly.
Following these guidelines will help ensure that the Prescription Pad form is used effectively and safely.
Other PDF Templates
Imm 1294 Form 2023 Pdf Download - Witnessing abuse or criminal activity requires disclosure on the form.
To facilitate the process of buying or selling a vehicle in Texas, you may find it helpful to use a template for the Texas Motor Vehicle Bill of Sale. This ensures that all necessary information is accurately captured and legally binding. For a convenient option, you can access a free template on Texas Forms Online, which can simplify the transaction for both parties involved.
Sex Yes No Maybe List - Open to using Saran wrap for sensory play.
Soccer Training Session Plan - Introduce passing techniques to enhance teamwork.
Example - Prescription Pad Form
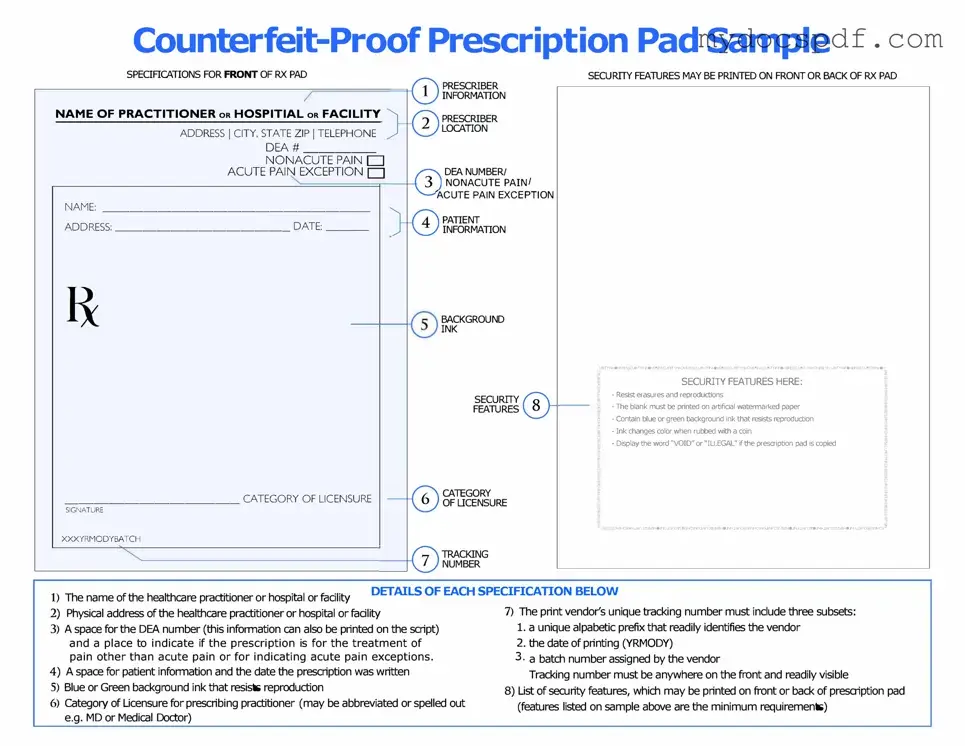
SPECIFICATIONS FOR FRONT OF RX PAD
NAME OF PRACTITIONER oR HOSPITIAL oR FACILITY
ADDRESS I CITY, STATE ZIP I TELEPHONE
DEA# _____□
NONACUTE PAIN
ACUTE PAIN EXCEPTION D
NAME: ___________________
ADDRESS: _____________ DATE: ___
____________ CATEGORY OF LICENSURE
SIGNATURE
XXXYRMODYBATCH
PRESCRIBER
INFORMATION
PRESCRIBER
LOCATION
DEA NUMBER/ NONACUTE PAIN/
ACUTE PAIN EXCEPTION
PATIENT
INFORMATION
BACKGROUND
INK
SECURITY
FEAllJRES
CATEGORY
OF LICENSURE
SECURITY FEAllJRES MAY BE PRINTED ON FRONT OR BACK OF RX PAD
� |
SECURITY FEAllJRES HERE: |
!i, |
|
|
|
|
- Resist erasures and reproductions |
|
|
- The blank must be printed on artificial waterrnarl<ed paper |
|
|
- Contain blue or green background ink that resists reproduction |
|
|
- Ink changes color when rubbed with a coin |
|
|
- Display the word "VOID" or"IU.EGAL" ifthe prescription pad is copied |
� |
|
|
_10HOJNIAl.nn::HS3'd3HOcJNl,Url!nJ=
1) |
The name of the healthc.are practitioner or hospital or facility |
DETAILS OF EACH SPECIFICATION BELOW |
|
|
7) The print vendor's unique tracking number must include three subsets: |
||
2) |
Physic.al address of the healthc.are practitioner or hospital or facility |
||
3) |
A space for the DEA number (this information c.an also be printed on the script) |
1. a unique alpabetic prefix that readily identifies the vendor |
|
|
and a place to indicate if the prescription is for the treatment of |
2. the date of printing (YRMODY) |
|
|
pain other than acute pain or for indicating acute pain exceptions. |
3 • a batch number assigned by the vendor |
|
4) |
A space for patient information and the date the prescription was written |
Tracking number must be anywhere on the front and readily visible |
|
5) |
Blue or Green background ink that resists reproduction |
|
8) List of security features, which may be printed on front or back of prescription pad |
6) |
Category of Licensure for prescribing practitioner (may be abbreviated or spelled out |
(features listed on sample above are the minimum requirements) |
|
|
e.g. MD or Medic.al Doctor) |
|
|
Detailed Instructions for Writing Prescription Pad
Completing the Prescription Pad form is an essential step in ensuring that patients receive their medications accurately. Properly filling out this form can help prevent errors and ensure that the necessary information is conveyed to the pharmacy. Follow these steps to complete the form effectively.
- Begin by entering the patient's full name at the top of the form.
- Next, write the patient's date of birth to help verify their identity.
- Indicate the patient's address, including street, city, state, and zip code.
- Specify the date when the prescription is being written.
- Clearly write the name of the medication being prescribed, including the dosage and form (e.g., tablet, liquid).
- Include the quantity of medication to be dispensed.
- Indicate the directions for use, detailing how and when the patient should take the medication.
- If necessary, note any refills authorized for the prescription.
- Sign the form with your full name and include your professional title.
- Finally, provide your contact information in case the pharmacy needs to reach you for clarification.
Documents used along the form
When managing prescriptions, several forms and documents may be necessary to ensure proper documentation and compliance. Below is a list of commonly used forms that often accompany the Prescription Pad form. Each document serves a specific purpose in the prescription process.
- Patient Information Form: This document collects essential details about the patient, including contact information, medical history, and allergies.
- Medication History Form: A record of all medications the patient has taken in the past, helping healthcare providers avoid potential drug interactions.
- Consent Form: A signed agreement from the patient, allowing the healthcare provider to prescribe medication and share medical information as needed.
- Insurance Information Form: This form captures the patient's insurance details to facilitate billing and ensure coverage for prescribed medications.
- Prescription Drug Monitoring Program (PDMP) Report: A report that tracks the patient's prescription history to prevent misuse and ensure safe prescribing practices.
- Refill Authorization Request: A request form used when a patient needs additional refills for their prescribed medication.
- Prior Authorization Form: A document required by some insurance companies to approve coverage for specific medications before they can be prescribed.
- Residential Lease Agreement: A https://newyorkform.com/free-residential-lease-agreement-template is essential for outlining the terms and conditions of renting residential property, ensuring clarity and protection for landlords and tenants alike.
- Controlled Substance Agreement: An agreement outlining the responsibilities of both the patient and the provider when prescribing controlled substances.
- Medication Administration Record (MAR): A log that tracks the administration of medications to the patient, ensuring compliance with the prescribed regimen.
Utilizing these documents alongside the Prescription Pad form can streamline the prescription process and enhance patient care. Ensure that all forms are completed accurately and kept up to date to maintain compliance and support effective communication between healthcare providers and patients.