Get Medication Error Form in PDF
The Medication Error form is a crucial tool designed to enhance patient safety and improve the quality of care in healthcare settings. This form is utilized for reporting all medication incidents, which include both errors in medication administration and discrepancies that may arise during the prescribing or dispensing processes. It is initiated by the pharmacist who discovers the error and requires immediate notification of the physician and pharmacy manager, especially in cases where a patient’s health or safety could be compromised. The form captures essential patient information, such as name, address, and date of birth, along with details about the medication involved, including the drug name, dosage, and the nature of the incident. It distinguishes between a medication incident, which directly affects a patient, and a medication discrepancy, which does not. Furthermore, the form includes sections for detailing the type of incident, contributing factors, and the severity of the error, allowing for a comprehensive investigation and follow-up. By systematically documenting these occurrences, healthcare providers can identify patterns, implement corrective actions, and ultimately reduce the likelihood of future medication errors.
Dos and Don'ts
When filling out the Medication Error form, it is crucial to follow specific guidelines to ensure accuracy and clarity. Below is a list of things you should and shouldn’t do.
- Do provide complete patient information, including name, address, and phone number.
- Do clearly state the type of incident or discrepancy.
- Do notify the physician and pharmacy manager of all incidents that could affect patient health.
- Do document the facts as known at the time of discovery.
- Don't omit any details regarding the error or incident.
- Don't delay in reporting the incident to ensure timely action.
- Don't use vague language; be specific in your descriptions.
- Don't forget to sign and date the form after completion.
Document Attributes
| Fact Name | Description |
|---|---|
| Purpose of the Form | This form is used to report all medication incidents, including discrepancies, at the discretion of the pharmacist. It serves to ensure patient safety and improve medication management practices. |
| Initiation of Report | The pharmacist who discovers the medication error is responsible for initiating the report. This emphasizes the importance of accountability in the medication management process. |
| Notification Requirements | All medication incidents that could affect a patient's health or safety must be reported to both the physician and the pharmacy manager. This ensures that all relevant parties are informed and can take appropriate action. |
| Types of Incidents | The form allows for the reporting of various types of incidents, such as incorrect dosage, allergic reactions, and drug interactions. Each incident type is clearly defined to facilitate accurate reporting. |
Key takeaways
- Use the form for all medication incidents. This includes discrepancies that pharmacists may report at their discretion.
- Initiate the report immediately. The pharmacist who discovers the error is responsible for starting the report.
- Notify key individuals. Inform both the physician and the pharmacy manager about any medication incidents that could impact patient health or safety.
- Provide accurate patient information. Include essential details such as name, address, phone number, date of birth, and prescription number.
- Clearly describe the incident. State the facts known at the time of discovery and attach any additional details if necessary.
- Complete the contributing factors section. Identify issues like improper patient identification or misinterpreted drug orders that led to the error.
Other PDF Templates
Peco Energy - PECO reserves the right to cancel requests lacking communication for 90 days.
Light Bill Template - Utilize this form for utility grant applications.
For a thorough understanding of the rental process, the important aspects of the Residential Lease Agreement must be reviewed, as it lays out the responsibilities and rights of both landlords and tenants in an Arizona rental situation.
Va 10-2850c - The form supports the VA's mission to provide quality care.
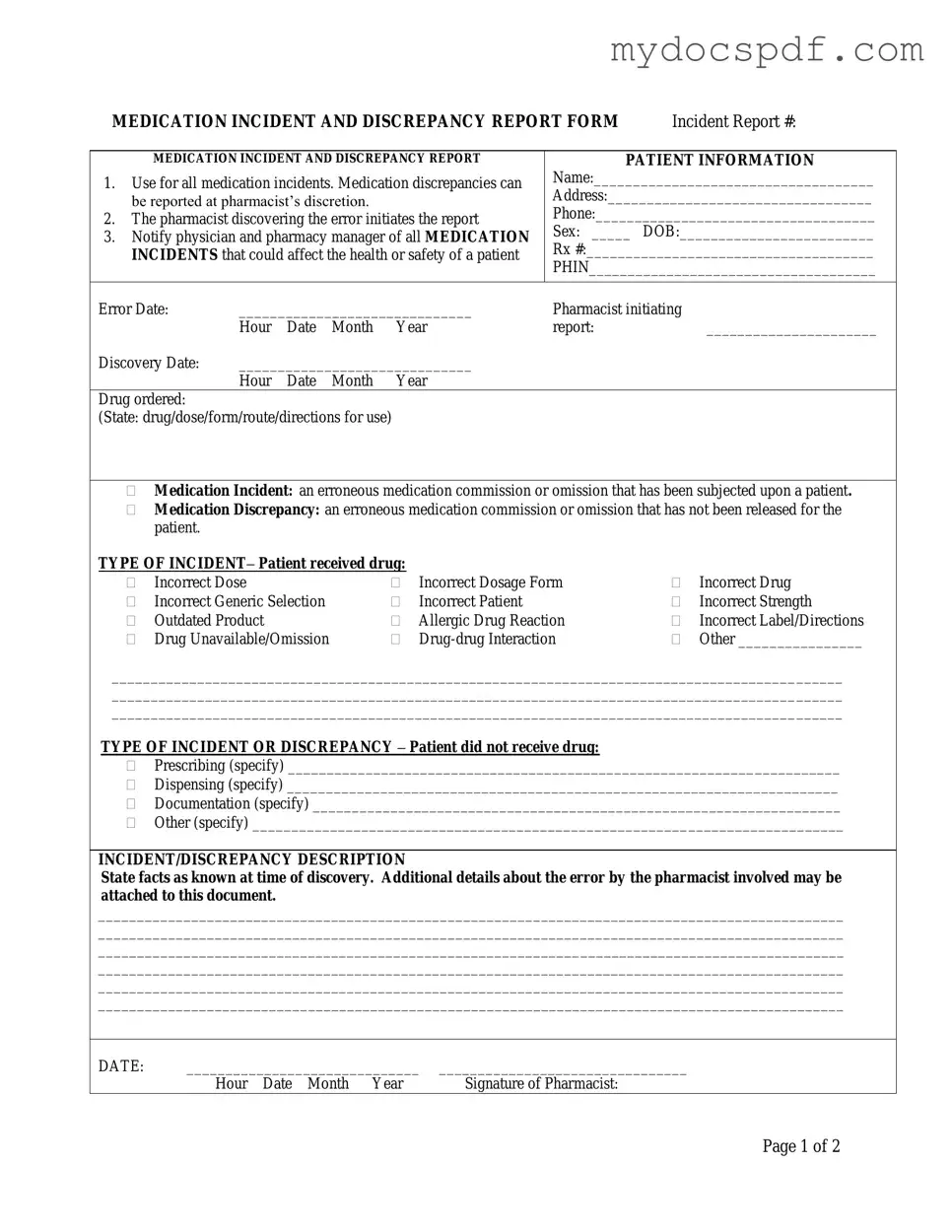
Example - Medication Error Form
MEDICATION INCIDENT AND DISCREPANCY REPORT FORM |
Incident Report #: |
MEDICATION INCIDENT AND DISCREPANCY REPORT
1.Use for all medication incidents. Medication discrepancies can be reported at pharmacist’s discretion.
2.The pharmacist discovering the error initiates the report
3.Notify physician and pharmacy manager of all MEDICATION INCIDENTS that could affect the health or safety of a patient
PATIENT INFORMATION
Name:____________________________________
Address:__________________________________
Phone:____________________________________
Sex: _____ DOB:_________________________
Rx #:_____________________________________
PHIN_____________________________________
Error Date: |
______________________________ |
Pharmacist initiating |
|
|||
|
Hour |
Date |
Month |
Year |
report: |
______________________ |
Discovery Date: |
______________________________ |
|
|
|||
|
Hour |
Date |
Month |
Year |
|
|
Drug ordered: |
|
|
|
|
|
|
(State: drug/dose/form/route/directions for use) |
|
|
|
|||
Medication Incident: an erroneous medication commission or omission that has been subjected upon a patient.
Medication Discrepancy: an erroneous medication commission or omission that has not been released for the patient.
TYPE OF INCIDENT– Patient received drug: |
|
|
|
||
|
Incorrect Dose |
|
Incorrect Dosage Form |
|
Incorrect Drug |
|
Incorrect Generic Selection |
|
Incorrect Patient |
|
Incorrect Strength |
|
Outdated Product |
|
Allergic Drug Reaction |
|
Incorrect Label/Directions |
|
Drug Unavailable/Omission |
|
|
Other ________________ |
|
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
TYPE OF INCIDENT OR DISCREPANCY – Patient did not receive drug:
Prescribing (specify) _______________________________________________________________________
Dispensing (specify) _______________________________________________________________________
Documentation (specify) ____________________________________________________________________
Other (specify) ____________________________________________________________________________
INCIDENT/DISCREPANCY DESCRIPTION
State facts as known at time of discovery. Additional details about the error by the pharmacist involved may be attached to this document.
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
DATE: |
______________________________ |
________________________________ |
|
Hour Date Month Year |
Signature of Pharmacist: |
Page 1 of 2
CONTRIBUTING FACTORS
(To be completed by pharmacist responsible)
|
Improper patient identification |
Misread/misinterpreted drug order (include verbal orders) |
|
|
Incorrect transcription |
|
Drug unavailable |
Lack of patient counselling |
|
Other |
|
|
DATE: |
______________________________ |
__________________ |
|
|
||||
|
|
Hour Date Month Year |
Signature |
|
|
|
|||
|
NOTIFICATION – Complete the following information according to Standards of Practice. |
||||||||
1. |
Patient notified: |
|
|
|
|
|
|
|
|
|
|
|
___________________________ |
|
|||||
|
|
|
Hour |
Date |
Month |
Year |
|||
2. |
Physician notified: ____ |
______________________________ |
|
||||||
|
|
Yes/No |
Hour |
Date |
Month |
Year |
|||
|
|
|
|
|
|
|
|
|
|
|
SEVERITY |
|
|
|
|
|
|
|
|
|
|
None |
|
No change in patient’s condition: no medical intervention |
|||||
|
|
Minor |
|
|
|
required |
|
|
|
|
|
Major |
|
Produces a temporary systemic or localized response: does |
|||||
|
|
|
|
|
|
not cause ongoing complications |
|||
|
|
|
|
Requires immediate medical intervention |
|||||
|
OUTCOME OF INVESTIGATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Problem Identification |
|
|
|
Action |
|
|
|
|
|
|
Lack of knowledge |
|
|
Education provided |
||||
|
|
Performance problem |
|
|
Policy/procedure changed |
||||
|
|
Administration problem |
|
|
System changed |
|
|
||
|
|
Other |
|
|
Individual awareness |
||||
|
|
|
|
|
Group awareness |
||||
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|||||
|
RESOLUTION OF PROBLEM THAT RESULTED IN THE ERROR BEING MADE: |
||||||||
|
|
|
|
|
|
|
|
||
|
Signature: |
Date: |
Signature: |
Date: |
|||||
|
(Pharmacist filling out the form) |
|
|
|
(Pharmacy Manager) |
||||
PHARMACY USE ONLY
Page 2 of 2
Detailed Instructions for Writing Medication Error
Completing the Medication Error form is an essential step in addressing medication incidents and discrepancies. After filling out the form, it will be submitted to the appropriate authorities for further action and review. This process ensures that necessary measures are taken to improve patient safety and prevent future occurrences.
- Incident Report Number: Write the incident report number at the top of the form.
- Patient Information: Fill in the patient's name, address, phone number, sex, date of birth, prescription number, and PHIN.
- Error Date: Enter the date of the medication error.
- Pharmacist Initiating Report: Provide your name and the date and time you discovered the error.
- Discovery Date: Fill in the date you discovered the error.
- Drug Ordered: Specify the drug, dose, form, route, and directions for use.
- Type of Incident: Indicate whether the patient received the drug and select the appropriate incident type from the list provided.
- Type of Incident or Discrepancy: If the patient did not receive the drug, specify the reason for the discrepancy.
- Incident/Discrepancy Description: Clearly describe the facts as known at the time of discovery. Include any additional details if necessary.
- Contributing Factors: Check any contributing factors that apply to the incident.
- Notification: Document whether the patient and physician were notified, including the date and time of notification.
- Severity: Indicate the severity of the incident based on the options provided.
- Outcome of Investigation Follow-Up: Record any problems identified and actions taken to resolve them.
- Signatures: Sign and date the form as the pharmacist filling it out and have the pharmacy manager sign and date as well.
Documents used along the form
The Medication Error form is an essential document used to report incidents related to medication discrepancies and errors. Several other forms and documents often accompany this report to ensure thorough communication and resolution of issues. Below is a list of related forms that may be utilized in conjunction with the Medication Error form.
- Incident Report Form: This form is used to document any unexpected events or incidents that occur within a healthcare setting. It provides a detailed account of the incident, including the individuals involved and any immediate actions taken.
- Patient Safety Report: This report focuses on incidents that may compromise patient safety. It aims to identify risks and enhance safety protocols within the healthcare environment.
- Pharmacy Audit Form: This form is utilized during audits to review medication dispensing processes. It helps ensure compliance with regulations and identifies areas for improvement in pharmacy operations.
- Medication Administration Record (MAR): The MAR is a detailed record of all medications administered to a patient. It includes information on dosages, times, and the person administering the medication, providing a clear history of medication use.
- Root Cause Analysis (RCA) Form: This document is used to investigate the underlying causes of a medication error or incident. It aims to identify systemic issues that contributed to the error and recommend preventive measures.
- Power of Attorney Form: A crucial document that allows individuals to appoint someone to manage their financial or legal matters in their absence. Understanding its implications is vital for proper management of personal affairs, similar to how a NY Templates can streamline the process of creating this form.
- Patient Notification Form: This form is used to document communication with the patient regarding any medication errors or discrepancies. It includes details about what occurred and the steps taken to address the situation.
- Quality Improvement Plan: This document outlines strategies for improving medication safety and reducing errors. It includes goals, actions, and timelines for implementing changes within the pharmacy or healthcare facility.
These forms and documents work together to enhance patient safety and improve medication management processes. Each one plays a vital role in ensuring that medication errors are addressed effectively and that systems are in place to prevent future incidents.