Get CMS-1763 Exp Form in PDF
The CMS-1763 Exp form plays a crucial role in the healthcare landscape, particularly for individuals seeking to maintain their Medicare coverage. This form is primarily used to request an extension of the Medicare enrollment period, allowing beneficiaries additional time to enroll without facing penalties. It serves as a vital tool for those who may have missed the initial enrollment window due to various circumstances, such as health issues or lack of awareness. Understanding the requirements and implications of the CMS-1763 Exp form is essential for beneficiaries to ensure they receive the healthcare benefits they deserve. The form requires specific information, including personal details and reasons for the extension request, and it must be submitted within a designated timeframe. By navigating this process effectively, individuals can secure their access to Medicare services and avoid potential gaps in their healthcare coverage.
Dos and Don'ts
When filling out the CMS-1763 Exp form, it's important to approach the process with care. Here are ten things to keep in mind, including what to do and what to avoid.
- Do: Read the instructions thoroughly before you start.
- Do: Ensure all personal information is accurate and up to date.
- Do: Use clear and legible handwriting if filling out the form by hand.
- Do: Double-check your entries for any potential errors.
- Do: Sign and date the form where required.
- Don't: Leave any required fields blank.
- Don't: Use correction fluid or tape on the form.
- Don't: Submit the form without making a copy for your records.
- Don't: Forget to include any supporting documents if necessary.
- Don't: Rush through the process; take your time to ensure accuracy.
By following these guidelines, you can help ensure that your CMS-1763 Exp form is completed correctly and processed smoothly.
Document Attributes
| Fact Name | Description |
|---|---|
| Form Purpose | The CMS-1763 Exp form is used to request a termination of Medicare coverage. |
| Eligibility | Individuals eligible for Medicare can use this form if they wish to end their coverage. |
| Submission Method | The completed form must be submitted to the Social Security Administration (SSA) or the local Medicare office. |
| Processing Time | Typically, processing takes 30 days from the date the form is received. |
| State-Specific Forms | Some states may have additional requirements or forms based on local laws regarding Medicare. |
| Governing Laws | Medicare is governed by federal laws, primarily the Social Security Act and related regulations. |
Key takeaways
Filling out the CMS-1763 Exp form can be straightforward if you keep a few key points in mind. Here are some important takeaways to help you navigate the process:
- Understand the purpose of the form. The CMS-1763 Exp form is used to request a termination of Medicare coverage.
- Gather necessary information before starting. You will need personal details, including your Medicare number and contact information.
- Be clear and concise in your responses. Providing accurate information helps avoid delays in processing your request.
- Double-check for errors. Review the form for any mistakes before submitting it to ensure it is complete and correct.
- Submit the form on time. Pay attention to deadlines to avoid any gaps in your Medicare coverage.
- Keep a copy of the completed form. This will serve as your record of the request and can be useful for future reference.
- Follow up if necessary. If you do not receive confirmation of your request, reach out to Medicare for updates.
Other PDF Templates
Invoice Form Pdf - Stay on top of your business finances with organized invoice tracking.
When entering into a lease, it is essential for both parties to understand the implications of a New York Residential Lease Agreement, which serves as a comprehensive contract detailing not only the rent amount and payment deadlines but also the duration of the lease. For those seeking clarity in their rental arrangements, you can find a useful template at newyorkform.com/free-residential-lease-agreement-template.
What Does the S in S Corp Stand for - The form outlines the necessary steps for an S corporation election.
Example - CMS-1763 Exp Form

DEPARTMENT OF HEALTH AND HUMAN SERVICES |
Form Approved |
CENTERS FOR MEDICARE & MEDICAID SERVICES |
OMB No. |
|
Expires: 04/24 |
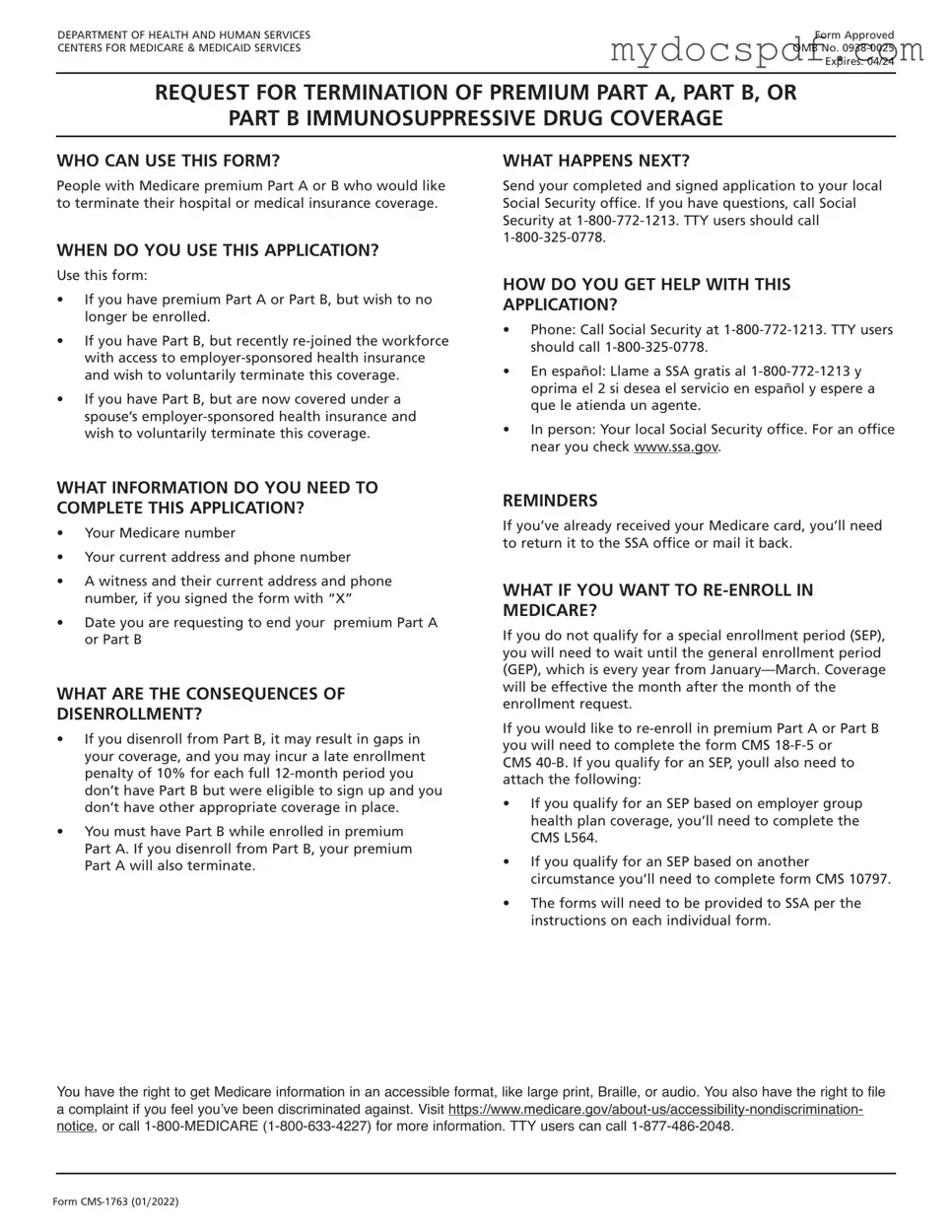
REQUEST FOR TERMINATION OF PREMIUM PART A, PART B, OR
PART B IMMUNOSUPPRESSIVE DRUG COVERAGE
WHO CAN USE THIS FORM?
People with Medicare premium Part A or B who would like to terminate their hospital or medical insurance coverage.
WHEN DO YOU USE THIS APPLICATION?
Use this form:
•If you have premium Part A or Part B, but wish to no longer be enrolled.
•If you have Part B, but recently
•If you have Part B, but are now covered under a spouse’s
WHAT HAPPENS NEXT?
Send your completed and signed application to your local Social Security office. If you have questions, call Social Security at
HOW DO YOU GET HELP WITH THIS
APPLICATION?
•Phone: Call Social Security at
•En español: Llame a SSA gratis al
•In person: Your local Social Security office. For an office near you check www.ssa.gov.
WHAT INFORMATION DO YOU NEED TO COMPLETE THIS APPLICATION?
•Your Medicare number
•Your current address and phone number
•A witness and their current address and phone number, if you signed the form with “X”
•Date you are requesting to end your premium Part A or Part B
WHAT ARE THE CONSEQUENCES OF
DISENROLLMENT?
•If you disenroll from Part B, it may result in gaps in your coverage, and you may incur a late enrollment penalty of 10% for each full
•You must have Part B while enrolled in premium Part A. If you disenroll from Part B, your premium Part A will also terminate.
REMINDERS
If you’ve already received your Medicare card, you’ll need to return it to the SSA office or mail it back.
WHAT IF YOU WANT TO
If you do not qualify for a special enrollment period (SEP), you will need to wait until the general enrollment period (GEP), which is every year from
If you would like to
CMS
•If you qualify for an SEP based on employer group health plan coverage, you’ll need to complete the CMS L564.
•If you qualify for an SEP based on another circumstance you’ll need to complete form CMS 10797.
•The forms will need to be provided to SSA per the instructions on each individual form.
You have the right to get Medicare information in an accessible format, like large print, Braille, or audio. You also have the right to file a complaint if you feel you’ve been discriminated against. Visit
Form
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
REQUEST FOR TERMINATION OF PREMIUM PART A, PART B,
OR PART B IMMUNOSUPPRESSIVE DRUG COVERAGE
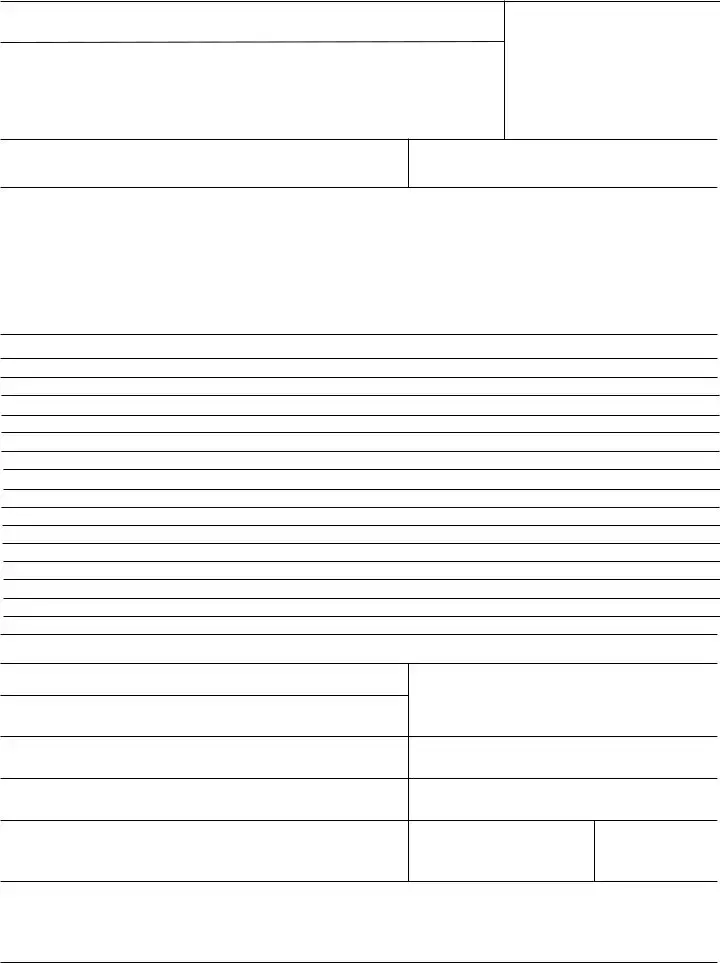
The completion of this form is needed to document your voluntary request for termination of Medicare coverage as permitted under the Code of Federal Regulations. Section 1838(b) and 1818A(c)(2)(B) of the Social Security Act require filing of notice advising the Administration when termination of Medicare coverage is requested. While you are not required to give your reasons for requesting termination, the information given will be used to document your understanding of the effects of your request.
DO NOT WRITE IN THIS SPACE
NAME OF ENROLLEE (Please Print)
MEDICARE NUMBER
NAME OF PERSON, IF OTHER THAN ENROLLEE, WHO IS EXECUTING THIS REQUEST.
THIS IS A REQUEST FOR TERMINATION OF |
DATE PART A |
DATE PART B |
DATE PBID |
HOSPITAL INSURANCE |
WILL END |
WILL END |
WILL END |
MEDICAL INSURANCE |
|
|
|
PART B IMMUNOSUPPRESSIVE DRUG COVERAGE |
|
|
|
|
|
|
|
I request termination of my enrollment under the above sections of title XVIII of the Social Security Act, as amended, for the reason(s) stated below:
I UNDERSTAND THAT IF I AM REQUIRED TO PAY FOR MY HOSPITAL INSURANCE, THE TERMINATION OF MY PART B COVERAGE WILL ALSO END MY PART A COVERAGE.
If this request has been signed by mark (X), two witnesses who know the applicant must sign below, giving their full addresses.
1. NAME OF WITNESS
SIGNATURE (Write in Ink)
SIGN
HERE
ADDRESS (Number and Street, City, State and Zip Code)
MAILING ADDRESS (Number and Street)
2. NAME OF WITNESS
CITY, STATE, ZIP CODE
ADDRESS (Number and Street, City, State and Zip Code)
DATE (Month, Day and Year)
TELEPHONE NUMBER
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
Form
Detailed Instructions for Writing CMS-1763 Exp
After obtaining the CMS-1763 Exp form, you will need to carefully complete it to ensure that all necessary information is accurately provided. This form requires personal details and specific information pertinent to your situation. Once filled out, you will submit the form to the appropriate agency for processing.
- Begin by entering your full name in the designated space at the top of the form.
- Provide your Social Security number, ensuring that it is accurate and legible.
- Fill in your date of birth in the specified format, typically MM/DD/YYYY.
- Next, indicate your current address, including street, city, state, and zip code.
- In the following section, provide your phone number. Include the area code for clarity.
- Complete the section regarding your Medicare information, including your Medicare number if applicable.
- Answer any additional questions as prompted, ensuring you read each question carefully.
- Review the entire form for accuracy and completeness before signing and dating it at the bottom.
- Finally, submit the completed form to the appropriate address as indicated in the instructions.
Documents used along the form
The CMS-1763 Exp form is an important document used in the context of Medicare. It allows individuals to request a termination of their Medicare coverage. Alongside this form, there are several other documents that may be needed to ensure a smooth process. Here’s a brief overview of some commonly used forms and documents that complement the CMS-1763 Exp form.
- CMS-10106: This is the "Medicare Enrollment Application." It is used by individuals who wish to enroll in Medicare, providing essential information about the applicant’s eligibility and personal details.
- Hold Harmless Agreement Form: This legal document is essential for protecting parties from liability for injuries or damages that may arise during specific activities. For further guidance, you can refer to Texas Forms Online for templates and resources.
- CMS-40B: Known as the "Application for Enrollment in Medicare Part B," this form is specifically for those looking to sign up for Medicare Part B. It requires information about the applicant’s current health insurance and coverage status.
- CMS-855I: This is the "Medicare Enrollment Application for Physicians and Non-Physician Practitioners." It’s used by healthcare providers to enroll in Medicare and includes details about their practice and services offered.
- CMS-1763: The original version of the CMS-1763 Exp form, which is used to request a termination of Medicare coverage. The distinction between the two is often in the context of the type of coverage being terminated.
- Form SSA-561-U2: This is the "Request for Reconsideration" form. If a Medicare coverage decision is disputed, this form allows individuals to appeal that decision and request a review.
- Form CMS-1500: This is the "Health Insurance Claim Form" used by healthcare providers to bill Medicare for services rendered. It includes information about the patient, the provider, and the services provided.
Each of these documents plays a crucial role in the Medicare process, whether it’s enrolling, terminating, or appealing a decision. Having the right forms ready can make a significant difference in ensuring that everything goes smoothly.