Get Advance Beneficiary Notice of Non-coverage Form in PDF
The Advance Beneficiary Notice of Non-coverage (ABN) form plays a crucial role in the landscape of healthcare services, particularly for Medicare beneficiaries. This important document serves as a notification to patients when a healthcare provider believes that a specific service or item may not be covered by Medicare. By providing this notice, providers aim to ensure that patients are fully informed about their potential financial responsibilities before receiving care. The ABN outlines the reasons for the anticipated non-coverage, allowing beneficiaries to make informed decisions about their treatment options. It also includes a space for patients to indicate whether they wish to proceed with the service despite the lack of guaranteed coverage. Understanding the implications of the ABN is essential for both patients and providers, as it fosters transparency and helps mitigate unexpected medical bills. Furthermore, the form emphasizes the importance of communication between patients and healthcare providers, ensuring that beneficiaries are not left in the dark about their rights and responsibilities regarding Medicare coverage.
Dos and Don'ts
When filling out the Advance Beneficiary Notice of Non-coverage (ABN) form, it is essential to approach the task with care. Here are eight important dos and don'ts to guide you through the process.
- Do read the form carefully before filling it out.
- Do provide accurate information to avoid delays in processing.
- Do sign and date the form to confirm your understanding.
- Do keep a copy of the completed form for your records.
- Don't leave any required fields blank.
- Don't rush through the process; take your time to ensure clarity.
- Don't ignore instructions provided on the form.
- Don't submit the form without reviewing it for errors.
By following these guidelines, you can ensure that your submission is clear and effective, minimizing potential issues down the line.
Document Attributes
| Fact Name | Description |
|---|---|
| Purpose | The Advance Beneficiary Notice of Non-coverage (ABN) informs Medicare beneficiaries that a service may not be covered by Medicare. |
| Usage | Healthcare providers use the ABN to notify patients before providing services that might not be reimbursed. |
| Patient Rights | Patients have the right to refuse services after receiving an ABN, understanding that they may have to pay out-of-pocket. |
| Timing | The ABN must be presented before the service is rendered, allowing the patient to make an informed decision. |
| State Variations | Some states may have specific laws governing the use of the ABN; for example, California's Business and Professions Code may apply. |
| Signature Requirement | Patients must sign the ABN to acknowledge that they understand the potential for non-coverage. |
| Documentation | Providers must keep a copy of the signed ABN in the patient's medical record for compliance and auditing purposes. |
Key takeaways
The Advance Beneficiary Notice of Non-coverage (ABN) is an important document in the Medicare system. Understanding how to fill it out and use it effectively can help beneficiaries navigate their healthcare options. Here are some key takeaways regarding the ABN:
- The ABN is used to inform Medicare beneficiaries that a service may not be covered by Medicare.
- It allows beneficiaries to make informed decisions about whether to receive a service or forgo it.
- Providers must issue the ABN before delivering services that they believe may not be covered.
- Beneficiaries should carefully read the ABN to understand the potential costs they may incur.
- It is important to sign the ABN to acknowledge understanding of the potential non-coverage.
- Beneficiaries can choose to accept or refuse the service after receiving the ABN.
- Keep a copy of the signed ABN for personal records and future reference.
- Using the ABN does not guarantee payment; it merely informs beneficiaries of possible non-coverage.
- If a service is denied by Medicare, beneficiaries can appeal the decision if they believe it should be covered.
By understanding these key points, beneficiaries can better navigate their healthcare decisions and financial responsibilities.
Other PDF Templates
Physical Evaluation Form - The history section addresses both current health and potential risks for athletes.
In order to create a Power of Attorney that meets specific needs, individuals can utilize resources like Texas Forms Online to find templates and guidance, ensuring that their legal documents are both effective and compliant with state laws.
Divorce Forms Michigan - The document includes a notary section to verify the authenticity of signatures, adding legal credibility.
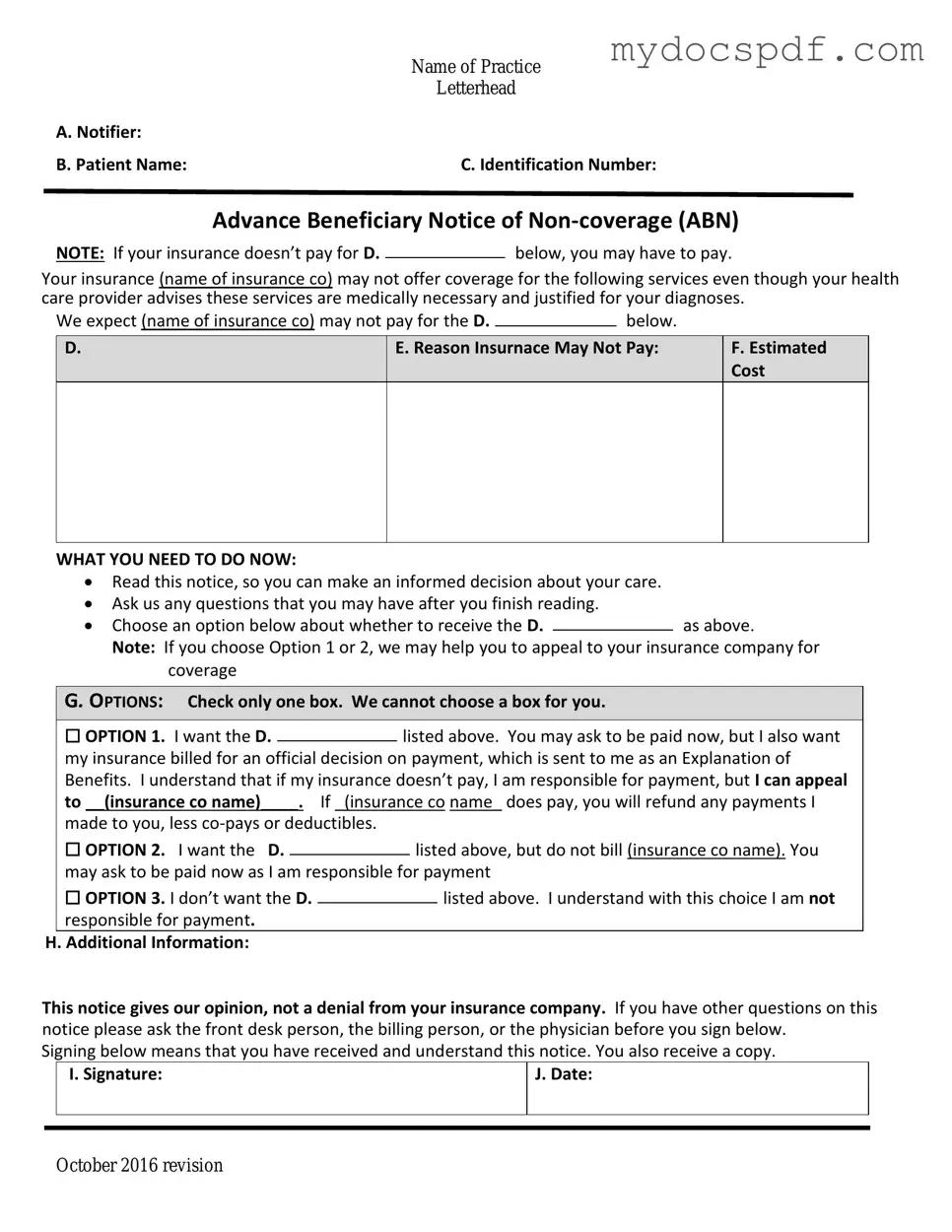
Example - Advance Beneficiary Notice of Non-coverage Form
|
Name of Practice |
|
Letterhead |
A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
Advance Beneficiary Notice of
NOTE: If your insurance doesn’t pay for D.below, you may have to pay.
Your insurance (name of insurance co) may not offer coverage for the following services even though your health care provider advises these services are medically necessary and justified for your diagnoses.
We expect (name of insurance co) may not pay for the D. |
|
below. |
|
D.
E. Reason Insurnace May Not Pay:
F.Estimated Cost
WHAT YOU NEED TO DO NOW:
Read this notice, so you can make an informed decision about your care.
Ask us any questions that you may have after you finish reading.
Choose an option below about whether to receive the D.as above.
Note: If you choose Option 1 or 2, we may help you to appeal to your insurance company for coverage
G. OPTIONS: Check only one box. We cannot choose a box for you.
|
☐ OPTION 1. I want the D. |
|
listed above. You may ask to be paid now, but I also want |
||||
|
|
||||||
|
my insurance billed for an official decision on payment, which is sent to me as an Explanation of |
||||||
|
Benefits. I understand that if my insurance doesn’t pay, I am responsible for payment, but I can appeal |
||||||
|
to __(insurance co name)____. If _(insurance co name_ does pay, you will refund any payments I |
||||||
|
made to you, less |
|
|
|
|||
|
☐ OPTION 2. I want the D. |
|
|
listed above, but do not bill (insurance co name). You |
|||
|
|
|
|||||
|
may ask to be paid now as I am responsible for payment |
||||||
|
☐ OPTION 3. I don’t want the D. |
|
|
|
listed above. I understand with this choice I am not |
||
|
|
|
|
||||
|
responsible for payment. |
|
|
|
|||
H. Additional Information: |
|
|
|
||||
This notice gives our opinion, not a denial from your insurance company. If you have other questions on this notice please ask the front desk person, the billing person, or the physician before you sign below.
Signing below means that you have received and understand this notice. You also receive a copy.
|
I. Signature: |
J. Date: |
|
|
|
|
|
|
October 2016 revision
Detailed Instructions for Writing Advance Beneficiary Notice of Non-coverage
Completing the Advance Beneficiary Notice of Non-coverage (ABN) form is a straightforward process that requires careful attention to detail. After filling out the form, you will be able to understand your financial responsibilities regarding certain healthcare services. This notice informs you that Medicare may not cover specific services, allowing you to make informed decisions about your care.
- Begin by entering the date at the top of the form.
- Fill in your name and Medicare number in the designated fields.
- Provide the name of the healthcare provider or facility that is issuing the notice.
- List the specific service or item that is being discussed in the notice.
- Clearly explain why the service may not be covered by Medicare in the provided section.
- Indicate whether you want to receive the service regardless of the potential lack of coverage.
- Sign and date the form at the bottom to acknowledge your understanding of the notice.
Documents used along the form
The Advance Beneficiary Notice of Non-coverage (ABN) is a crucial document that informs Medicare beneficiaries when a service may not be covered. However, several other forms and documents are commonly used in conjunction with the ABN to ensure clarity and compliance. Below is a list of these documents, each playing a significant role in the healthcare process.
- Medicare Summary Notice (MSN): This notice is sent to beneficiaries every three months and summarizes the services received, the amount billed, and the Medicare payment details. It helps patients understand what has been covered and what they may owe.
- Notice of Exclusions from Medicare Benefits (NEMB): This document explains the services that Medicare does not cover. It provides beneficiaries with information about exclusions, helping them make informed decisions regarding their healthcare options.
- Claim Form (CMS-1500 or UB-04): These forms are used by healthcare providers to submit claims for payment to Medicare. They detail the services provided and are essential for processing reimbursement.
- Homeschool Letter of Intent Form: For families planning to educate their children at home, learn about the important aspects of the Homeschool Letter of Intent requirements to ensure compliance with state regulations.
- Patient Consent Form: Before certain services are rendered, providers may require patients to sign a consent form. This document ensures that patients understand the nature of the services and agree to them.
- Advanced Care Planning Documents: These documents include living wills and healthcare proxies. They outline patients’ preferences for medical treatment in the event they cannot communicate their wishes, ensuring that their healthcare aligns with their values.
- Medicare Enrollment Application (CMS-855I): This form is used by healthcare providers to enroll in Medicare. It is essential for ensuring that providers can bill Medicare for services rendered.
- Financial Responsibility Agreement: This document outlines the financial obligations of the patient regarding services not covered by Medicare. It ensures transparency about potential out-of-pocket costs.
- Appeal Form: If a claim is denied, beneficiaries can use this form to appeal the decision. It is crucial for ensuring that patients have the opportunity to contest coverage denials.
Each of these documents serves a specific purpose in the healthcare landscape. Understanding their roles can empower beneficiaries to navigate their Medicare options more effectively and advocate for their rights. Familiarity with these forms can lead to a smoother healthcare experience and better outcomes.