Get Ada Dental Claim Form in PDF
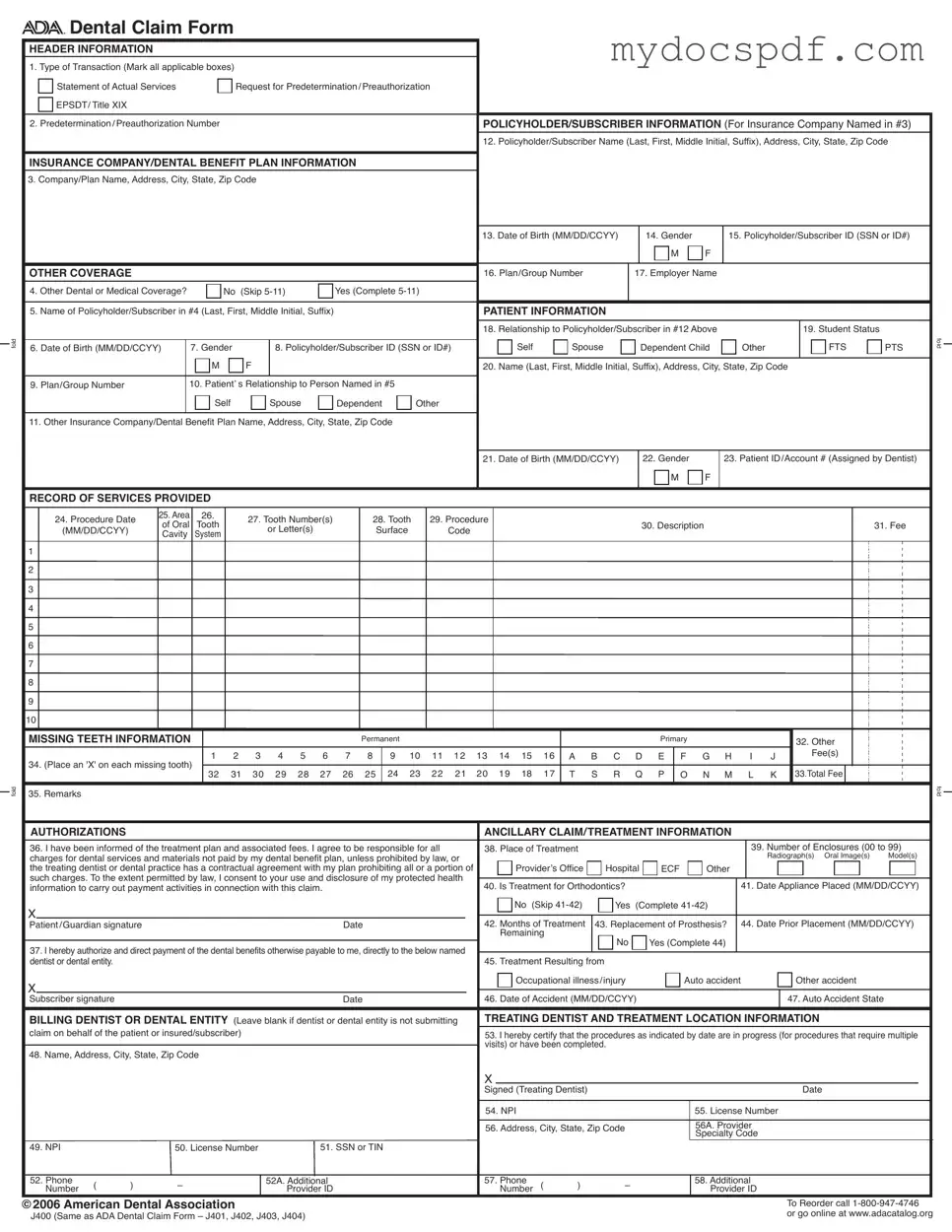
The ADA Dental Claim Form serves as a crucial tool in the realm of dental insurance, facilitating the process of submitting claims for reimbursement. This form encompasses a variety of essential sections, each designed to gather specific information necessary for processing claims efficiently. At the outset, users will find header information that prompts the completion of transaction types, such as requests for actual services or predetermination. Following this, detailed sections require the policyholder's and subscriber's information, ensuring that the correct insurance details are captured. Patient information is meticulously gathered, including relationships to the policyholder and student status, which can affect coverage eligibility. As the form progresses, it captures a comprehensive record of services provided, detailing procedure dates, tooth numbers, and associated fees. The inclusion of missing teeth information allows for a complete picture of the patient's dental health. Moreover, the form addresses authorizations and treatment specifics, ensuring that all parties are informed and agree to the treatment plan. Completing the form accurately is paramount, as it directly impacts the timely processing of claims and the benefits received by patients. Each section, from billing details to the treating dentist's information, plays a pivotal role in the overall efficiency of the claims process, making the ADA Dental Claim Form an indispensable component of dental practice management.
Dos and Don'ts
When filling out the ADA Dental Claim form, keep the following tips in mind:
- Do ensure all required fields are completed accurately.
- Don’t leave any sections blank unless specified.
- Do use the full name and address for policyholders and subscribers.
- Don’t abbreviate names or addresses.
- Do include the four-digit year for all dates.
- Don’t submit multiple claims on one form if there are more procedures than lines available.
- Do attach the primary payer’s Explanation of Benefits when submitting to a secondary payer.
- Don’t forget to sign and date the form before submission.
- Do fold the form properly to ensure visibility of the payer's information.
Document Attributes
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The ADA Dental Claim Form is used to submit dental claims for insurance reimbursement. |
| Header Information | It includes transaction types, such as actual services or preauthorization requests. |
| Policyholder Information | Details about the policyholder, including name and address, are required. |
| Patient Information | Information about the patient must be provided, including their relationship to the policyholder. |
| Record of Services | This section documents the dental procedures performed, including dates and fees. |
| Missing Teeth Information | Claimants must indicate any missing teeth using designated codes. |
| Authorization Section | Patients must sign to authorize payment and acknowledge understanding of treatment costs. |
| National Provider Identifier (NPI) | The form requires the NPI of the treating dentist, a unique identifier for healthcare providers. |
| Coordination of Benefits | If applicable, attach the primary payer's Explanation of Benefits when submitting to a secondary payer. |
| State-Specific Laws | Each state may have specific regulations that govern the use of this form in dental claims. |
Key takeaways
Filling out the ADA Dental Claim Form accurately is essential for ensuring timely processing of dental claims. Here are key takeaways to consider:
- Transaction Types: Clearly mark the applicable transaction types at the top of the form. This includes options such as 'Statement of Actual Services' and 'Request for Predetermination/Preauthorization.'
- Policyholder Information: Provide complete details about the policyholder, including their name, address, and date of birth. This information is critical for insurance verification.
- Other Coverage: If the patient has other dental or medical coverage, indicate this by completing the relevant sections. This ensures proper coordination of benefits.
- Patient Details: Accurately fill in the patient's relationship to the policyholder and their own personal information, including date of birth and gender.
- Record of Services: Document all services provided, including procedure dates, tooth numbers, and associated fees. This section must be completed thoroughly to avoid delays.
- Authorization: Obtain the necessary signatures from the patient or guardian to authorize payment and confirm understanding of the treatment plan and fees.
- National Provider Identifier (NPI): Ensure that the billing dentist's NPI is included. This identifier is crucial for processing claims in compliance with federal regulations.
- Additional Identifiers: If applicable, include any additional provider identifiers. These may be required by certain insurance companies for claim processing.
By following these guidelines, individuals can facilitate a smoother claims process and reduce the likelihood of errors or delays in reimbursement.
Other PDF Templates
Divorce Forms Michigan - The Michigan Complaint Divorce form is essential for any couple looking to formally end their marriage.
The California Release of Liability form is a legal document by which a person relinquishes their right to bring a lawsuit against another party for any injuries or damages suffered. This agreement is often used in situations where individuals participate in potentially hazardous activities or events. It serves as a crucial tool in managing legal risks and providing peace of mind for both parties involved. To ensure you have the correct documentation, you can refer to for the form.
Imm 5645 - Certification requires your signature and date at the end of the form.
Example - Ada Dental Claim Form
fold
fold



 Dental Claim Form
Dental Claim Form
HEADER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. Type of Transaction (Mark all applicable boxes) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Statement of Actual Services |
|
|
Request for Predetermination/Preauthorization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
EPSDT/ Title XIX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Predetermination/Preauthorization Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER/SUBSCRIBER INFORMATION (For Insurance Company Named in #3) |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
INSURANCE COMPANY/DENTAL BENEFIT PLAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Company/Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Date of Birth (MM/DD/CCYY) |
|
|
14. Gender |
|
|
15. Policyholder/Subscriber ID (SSN or ID#) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
OTHER COVERAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. Plan/Group Number |
|
|
17. Employer Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
4. Other Dental or Medical Coverage? |
|
|
No (Skip |
|
|
Yes (Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) |
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Relationship to Policyholder/Subscriber in #12 Above |
|
|
|
|
|
|
|
19. Student Status |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FTS |
PTS |
fold |
|||||||||
6. Date of Birth (MM/DD/CCYY) |
|
7. Gender |
|
|
|
8. Policyholder/Subscriber ID (SSN or ID#) |
|
|
|
Dependent Child |
Other |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
9. Plan/Group Number |
|
|
10. Patient’ s Relationship to Person Named in #5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Self |
|
|
|
Spouse |
|
Dependent |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. Date of Birth (MM/DD/CCYY) |
|
|
22. Gender |
|
|
23. Patient ID/Account # (Assigned by Dentist) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
RECORD OF SERVICES PROVIDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. Procedure Date |
25. Area |
26. |
|
27. Tooth Number(s) |
|
|
28. Tooth |
29. Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
of Oral |
Tooth |
|
|
|
|
|
|
|
|
|
30. Description |
|
|
|
|
|
|
|
|
|
|
|
31. Fee |
|
||||||||||||||||||||||||||||
|
(MM/DD/CCYY) |
|
|
|
|
or Letter(s) |
|
|
|
Surface |
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Cavity |
System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MISSING TEETH INFORMATION |
|
|
|
|
|
|
|
|
|
|
Permanent |
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
|
|
|
|
|
|
|
32. Other |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
8 |
|
9 10 11 12 13 14 15 16 |
A B C D E |
F G H |
|
I |
J |
|
|
|
|
Fee(s) |
|
|
|
|
|
|
|
|||||||||||||||||||
34. (Place an 'X' on each missing tooth) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
32 |
31 |
30 |
29 |
28 |
27 |
26 |
|
25 |
|
24 23 |
22 21 |
|
20 19 18 |
17 |
T |
S R |
Q |
P |
O |
N M |
|
L |
K 33.Total Fee |
|
|
|
|
|
|
|
||||||||||||||||
35. Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
fold |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
AUTHORIZATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANCILLARY CLAIM/TREATMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all |
38. Place of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
39. Number of Enclosures (00 to 99) |
|
||||||||||||||||||||||||||||||||||||||
charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Radiograph(s) Oral Image(s) |
Model(s) |
|
|||||||||||||||||||||||||||||||||
the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a portion of |
|
Provider’s Office |
Hospital |
ECF |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
information to carry out payment activities in connection with this claim. |
|
|
|
|
|
|
|
40. Is Treatment for Orthodontics? |
|
|
|
|
|
|
|
|
|
41. Date Appliance Placed (MM/DD/CCYY) |
|
||||||||||||||||||||||||||||||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No (Skip |
Yes |
(Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/Guardian signature |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
42. Months of Treatment |
43. Replacement of Prosthesis? |
|
44. Date Prior Placement (MM/DD/CCYY) |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named |
|
|
|
|
No |
|
|
Yes (Complete 44) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
dentist or dental entity. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. Treatment Resulting from |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupational illness/injury |
|
|
|
Auto accident |
|
|
|
|
|
Other accident |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber signature |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
46. Date of Accident (MM/DD/CCYY) |
|
|
|
|
|
|
|
|
|
|
47. Auto Accident State |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting |
TREATING DENTIST AND TREATMENT LOCATION INFORMATION |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
claim on behalf of the patient or insured/subscriber) |
|
|
|
|
|
|
|
|
|
|
|
|
|
53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require multiple |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
visits) or have been completed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
48. Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signed (Treating Dentist) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. NPI |
|
|
|
|
|
|
|
|
|
55. License Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
56. Address, City, State, Zip Code |
|
|
|
|
|
56A. Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
49. NPI |
|
|
50. License Number |
|
|
|
51. SSN or TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
52. Phone |
( |
) |
– |
|
|
|
|
|
52A. Additional |
|
|
|
|
|
|
|
57. Phone |
( |
) |
– |
|
|
|
|
|
58. Additional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Number |
|
|
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
©2006 American Dental Association |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Reorder call |
|
||||||||||||||||||||
J400 (Same as ADA Dental Claim Form – J401, J402, J403, J404) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or go online at www.adacatalog.org |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||

Comprehensive completion instructions for the ADA Dental Claim Form are found in Section 4 of the ADA Publication titled
GENERAL INSTRUCTIONS
A. The form is designed so that the name and address (Item 3) of the
B. In the
assignment of a claim or control number.
|
C. All Items in the form must be completed unless it is noted on the form or in the following instructions that completion is not required. |
|
|
D. When a name and address field is required, the full name of an individual or a full business name, address and zip code must be entered. |
|
|
E. All dates must include the |
|
|
F. If the number of procedures reported exceeds the number of lines available on one claim form, the remaining procedures must be |
|
listed on a separate, fully completed claim form. |
|
COORDINATION OF BENEFITS (COB)
When a claim is being submitted to the secondary payer, complete the form in its entirety and attach the primary payer’s Explanation of Benefits (EOB) showing the amount paid by the primary payer. You may indicate the amount the primary carrier paid in the “Remarks” field (Item # 35).
NATIONAL PROVIDER IDENTIFIER (NPI)
49 and 54 NPI (National Provider Indentifier): This is an identifier assigned by the Federal government to all providers considered to be HIPAA covered entities. Dentists who are not covered entities may elect to obtain an NPI at their discretion, or may be enumerated if required by a participating provider agreement with a
ADDITIONAL PROVIDER IDENTIFIER
52A and 58 Additional Provider ID: This is an identifier assigned to the billing dentist or dental entity other than a Social Security Number (SSN) or Tax Identification Number (TIN). It is not the provider’s NPI. The additional identifier is sometimes referred to as a Legacy Identifier (LID). LIDs may not be unique as they are assigned by different entities (e.g.,
PROVIDER SPECIALTY CODES
56A Provider Specialty Code: Enter the code that indicates the type of dental professional who delivered the treatment. Available codes describing treating dentists are listed below. The general code listed as ‘Dentist’ may be used instead of any other dental practitioner code.
Category / Description Code |
Code |
|
|
Dentist |
|
A dentist is a person qualified by a doctorate in dental surgery (D.D.S) |
122300000X |
or dental medicine (D.M.D.) licensed by the state to practice dentistry, |
|
and practicing within the scope of that license. |
|
|
|
General Practice |
1223G0001X |
Dental Specialty (see following list) |
Various |
Dental Public Health |
1223D0001X |
Endodontics |
1223E0200X |
Orthodontics |
1223X0400X |
Pediatric Dentistry |
1223P0221X |
Periodontics |
1223P0300X |
Prosthodontics |
1223P0700X |
Oral & Maxillofacial Pathology |
1223P0106X |
Oral & Maxillofacial Radiology |
1223D0008X |
Oral & Maxillofacial Surgery |
1223S0112X |
Dental provider taxonomy codes listed above are a subset of the full code set that is posted at:
Should there be any updates to ADA Dental Claim Form completion instructions, the updates will be posted on the ADA’s web site at:
www.ada.org/goto/dentalcode
Detailed Instructions for Writing Ada Dental Claim
Completing the ADA Dental Claim Form is a straightforward process that requires careful attention to detail. Each section of the form gathers specific information necessary for processing the claim. By following the steps outlined below, individuals can ensure that all required information is accurately provided, which will facilitate timely processing by the insurance company.
- Type of Transaction: Mark all applicable boxes in the header section, indicating whether it is a Statement of Actual Services, Request for Predetermination/Preauthorization, or EPSDT/Title XIX.
- Predetermination/Preauthorization Number: Fill in the number if applicable.
- Policyholder/Subscriber Information: Enter the name, address, city, state, and zip code of the policyholder or subscriber.
- Insurance Company/Dental Benefit Plan Information: Provide the company or plan name, address, city, state, and zip code.
- Date of Birth: Enter the policyholder/subscriber's date of birth in MM/DD/CCYY format.
- Gender: Indicate the gender of the policyholder/subscriber.
- Policyholder/Subscriber ID: Input the Social Security Number (SSN) or identification number.
- Other Coverage: If there is other dental or medical coverage, answer "Yes" and complete items 5-11; otherwise, skip to the patient information section.
- Name of Policyholder/Subscriber: If applicable, provide the name of the other policyholder/subscriber.
- Patient Information: Fill in the relationship to the policyholder/subscriber, student status, date of birth, gender, and ID/account number assigned by the dentist.
- Record of Services Provided: For each procedure, enter the date, area, tooth number(s), procedure code, description, and fee.
- Missing Teeth Information: Mark each missing tooth with an 'X' and calculate the total fee.
- Authorizations: Confirm understanding of the treatment plan and fees, and provide the patient or guardian's signature and date.
- Billing Dentist or Dental Entity: If applicable, fill in the name, address, and other identifiers of the billing dentist or dental entity.
- Treating Dentist and Treatment Location Information: Complete the treating dentist's information and sign to certify the procedures have been completed or are in progress.
Once the form is filled out completely, it should be submitted to the appropriate insurance company or dental benefit plan for processing. Ensure that all necessary documents, such as the primary payer's Explanation of Benefits, are included if applicable. This attention to detail will help in avoiding delays in claim processing.
Documents used along the form
When submitting a dental claim, several additional forms and documents may be required to ensure a smooth process. Each of these documents serves a specific purpose and helps provide necessary information to the insurance company or dental benefit plan.
- Explanation of Benefits (EOB): This document details the coverage provided by the insurance company. It includes information about what procedures were covered, the amounts paid, and any patient responsibility.
- Patient Registration Form: This form collects essential information about the patient, including personal details and insurance information. It is often completed at the first visit to a dental office.
- Authorization for Release of Information: This document allows the dental provider to share the patient's medical and dental records with the insurance company. It is crucial for processing claims efficiently.
- Referral Form: If a patient is referred to a specialist, this form provides the necessary details about the referral. It helps ensure that the specialist has all the information needed for treatment.
- Arizona Notice to Quit Form: This legal document is crucial for landlords in Arizona to formally notify tenants of the requirement to vacate the rental property. For more information, you can refer to arizonapdfs.com.
- Treatment Plan: This outlines the proposed dental treatments and associated costs. It is often required for preauthorization before certain procedures can be performed.
- Coordination of Benefits (COB) Form: When a patient has multiple insurance plans, this form helps determine which plan is primary and how benefits will be coordinated between them.
- Claim Appeal Form: If a claim is denied, this form is used to appeal the decision. It typically requires additional documentation or justification for the claim.
- Consent for Treatment Form: This document confirms that the patient understands and agrees to the proposed treatments. It is an important part of the patient’s record.
Having these documents ready can help streamline the claims process and reduce delays in receiving benefits. Each form plays a vital role in ensuring that both the patient and the provider are protected and informed throughout the dental treatment journey.